The criminal justice system (CJS) is broken. Not many would disagree with this; some say it’s too lenient, some think it’s too harsh, and others believe it is much more complicated than that. I am in the third group, and this is because I have seen both sides. As a person with lived experience, I would like to give my take on why the system, as it stands, is unjust and not fit for purpose. But first, a little background…
At the age of eighteen, I chased an abusive boyfriend into the street with a kitchen knife. After months of physical and psychological abuse, I finally snapped. I was charged with possession of an offensive weapon and given a conditional discharge. Thirty-six years later, I was charged with possession of a bladed instrument after a kitchen knife, which I used to cut up takeaway food for my disabled partner, was found in the back of my car. For this, I was given twelve months in prison.
Although I had not been in trouble during those thirty-six years, the judge decided that I had an affinity with knives, hence the custodial sentence. He was also influenced by the fact that I had borderline personality disorder (BPD) and had verbally abused my psychiatrist, whose incompetence had led me to believe for over a year that I was on a waiting list for treatment when, in fact, I wasn’t and never had been.
As a result of my ‘abuse’ of the psychiatrist, I was told that I would not now, nor in the foreseeable future, receive any help from the community mental health service (CMHS). This did not affect me too much; they seemed to know very little about BPD, and I knew I wouldn’t receive adequate treatment, even if they were willing. However, this lack of awareness was also obvious in court, to my detriment.
Anyone who has experienced a first night in prison will recognise the emotions that I went through. Desperation, claustrophobia, helplessness, hopelessness, guilt, shame, anger. All these emotions come together as soon as that thick metal door is closed. I would liken it to being thrown in a hole; in my case it was in an old army barracks, and it was cold and filthy. I could hear rats scurrying around outside, waiting for the prisoners’ leftover food that was regularly thrown to them out of the window.
My distress was evident but was inconsequential to the officers. One thing I learned quickly was that as soon as you enter prison, you are automatically seen as a liar, and an attention-seeker. On my fifth day, I sat on my bed and set fire to the mattress. I didn’t know at the time that prison officers are trained firefighters and the hose soon appeared in a hole in the door, put there for that very scenario. For this, I was given another twelve months in prison.
Sentencing
In my experience, and that of others I have spoken to, there is very little compassion among crown court judges when sentencing. Furthermore, sentences are inconsistent, which can lead to the individual feeling a sense of injustice and even bitterness. I feel this often when hearing about those who commit horrendous crimes and yet do not receive a sentence as harsh as mine. I accept responsibility for what I did. The knife was in my car for a valid reason, but it was illegal, and I paid the price. Arson is a serious crime and, although no-one was hurt, it could have got out of hand. I know that I was ill at the time, I certainly didn’t want to hurt anyone apart from myself, but it was wrong and, again, I paid the price.
UK judges are meant to look holistically at an offender when it comes to sentencing. How can they do that if they do not understand the reasons why the offence has been committed? The police detective in charge of my case insisted that I was ‘bad not mad’. Personally, I don’t think I am either, but people in authority do love a cliché! She was helped by the fact that BPD is highly stigmatised and misunderstood, and I truly believe that the judge was risk averse. What if he released me and I reoffended? He wasn’t taking the chance. In reality, there was far more chance of someone convicted for a violent crime reoffending than me.
There is evidence in some countries that individuals are more likely to be disposed of quicker and without much thought, if they appear in front of the judge in the afternoon, rather than the morning.[i] This phenomenon is called ‘decision fatigue’ and, although there have been no studies in the UK, I think it’s safe to say that it does happen here.
The court set-up
Regardless of the offence, the court set-up disadvantages the individual from the start. Although the holding cells differ between courts, many are extremely small, single cells with no natural light and not even enough bench space to lie down. If someone is appearing in the courtroom for a short time, they can be in that cell for seven or more hours, waiting for transport back to prison. These cells are extremely claustrophobic and there is no stimulation unless the custody officer is kind enough to offer a magazine. It can be tremendously distressing for the defendant and can affect their appearance in court.
After being taken up to the courtroom, the accused is seated in a box behind a sheet of glass that has a narrow slit in the middle. Even those without hearing problems can find it difficult to follow the conversation and this is further hindered by the fact that the barristers stand with their backs towards the box.
A typical American court will have the individual sitting with their defence team and so if they disagree with anything that is said, they can give a message to their team. This doesn’t happen in UK courts and so it often happens that by the time the defendant speaks to the barrister at the lunch break or at the end of the day, it is too late to argue the point.
There also seems to be a lack of thought for the individual when planning subsequent court appearances. I remember sitting in the box whilst the judge and my barrister discussed their respective diaries, trying to find a mutually available date. Every time they turned a page was extra time that I would be staying in prison. More expense for the taxpayer and more distress for me and my family.
Consequences of an inadequate CJS
The most obvious result of a broken system is financial; the enormous waste of money that is spent on sending people to prison instead of investing in preventative measures, such as better mental health care, accommodation, and other areas where people are subject to multiple disadvantages. Are we seen as collateral damage? Could the reason that the government fails to invest in prevention be because it is a long-term solution, and they need quicker outcomes in order to satisfy public opinion? A politician’s shelf-life is getting shorter, and they need that vote!
The most important consequence of sending people to prison unnecessarily is the long-term effect it has on those on remand/convicted, and their dependents. Children are likely to suffer trauma through their enforced separation form their parent(s) and in some cases, they are left alone with a father whose abuse, whether physical, coercive or some other form, has led directly to the mother being imprisoned. The children may be taken into care, meaning that when their parent gets released, there is no family home, leading to a long, traumatic process to bring the parent and child together gain.
Many people in prison are known to have at least one mental health condition. It is increasingly unlikely that they will get help for their problems, especially if they are serving a short sentence. For example, there are several personality disorder units in prison, but in order to access one the individual must have at least two years left to serve. The rest rely on prison services such as In-reach, usually a small team responsible for several hundred prisoners. Similarly, the various courses which address the individual’s crime and associated behaviour, and which are a main part of rehabilitation, are usually only available to those with a longer-term sentence.
A consequence of having an untreated mental health issue in prison is that the individual’s behaviour is not understood by the officers, and they are more likely to end up in segregation, isolated for twenty-three hours a day with very little stimulation. This has been called abhorrent and inhumane and can only exacerbate a mental health condition; it does not bode well for the individual when re-entering the community.
Is it madness?
The UK has the largest prison population in western Europe and the third largest in the whole of Europe. It also has the highest population of prisoners serving life sentences.[ii] Yet, recidivism is high, at around 50% for adults released from custodial sentences of less than twelve months.[iii] Reoffending is lower for those receiving community sentences, yet we continue to send people to prison for short sentences.
The true definition of madness is repeating the same action, over and over, hoping for a different result. Albert Einstein
There are many reports highlighting the ways in which the CJS is failing both victims and offenders and recommending alternatives. Some of them are given below. However, I will leave you with the story of someone I met in prison which is, I believe, a perfect example of a broken criminal justice system:
‘A’ had received 44 days in prison for non-payment of council tax. She told me that she was exempt from the payment because she was on benefits but had failed to fill in the correct form. Consequently, she was liable for the full amount, just over £2,000. She could be released at any time if her family were able to make the payment in full. ‘A’ was sixty years old, not much older than me, and was devastated at the position she had found herself in. She had never been in trouble before and was struggling to process what had happened. She suffered from migraines but was laughed at by the officers, who said she was attention-seeking.
The amount of money it cost the taxpayer to keep ‘A’ in prison for 44 days far outweighed the amount of arrears she owed. If her family couldn’t pay to get her released early, a repayment plan would be put in plan on her release and a small amount would be taken from her benefits each week. Surely, all this could have been done beforehand and the financial cost and distress caused by her sentence could have been avoided!
Perhaps common sense should direct sentencing, with more attention focused on those who commit violent crimes. Perhaps the money saved by not imprisoning people with mental health conditions, and those who commit minor crimes, could be spent in the community, on mental health and other preventative measures. And perhaps decision-makers should not focus on their own agenda, but on what is important, fairness and justice.
One person in 20 is currently living with a personality disorder and a large proportion of these are women. Symptoms vary but in Stacey’s case she struggled with her emotions and relationships with others. She feels strongly that probation officers need more training to enable them to understand the difficulties of working with people with personality disorders.
The first meeting with my probation officer started off badly. She had read my case notes which said I was ‘high risk’ and made it clear she had reservations about supervising me. I had Borderline Personality Disorder (BPD) and was known to struggle to manage my emotions. The Community Mental Health Team (CMHT) had refused to help me saying first that there was no treatment for BPD and then, after my arrest, that I was obviously in crisis and so unable to engage, so I was used to knock backs.
Nevertheless, I was a little disappointed with her attitude and the fact that she had pre-judged me. I had never had a probation officer before and didn’t know what to expect. I was 55 years old and this was my first time in prison. I was looking forward to going home to my partner and I was sure that I would not be returning to prison.
After my release I saw my probation officer twice a week. I attended all my appointments and didn’t offend further, so after a couple of months they were cut down to one a week. I wasn’t getting any help from the CMHT but it didn’t seem to matter because I could talk to my probation officer. She’d softened towards me since our initial meeting and I looked forward to seeing her each week.
We spoke about issues I was having but equally, we discussed her and her personal life.
“Enough about you, did I tell you about what I did last weekend?” she’d say.
I liked talking to her. She was funny, intelligent and interesting. She seemed to care about me. We discussed my issues with attachment, a common symptom of BPD, and she seemed to understand what a serious problem it was for me. The feelings can become so intense that some people become obsessed and even resort to stalking. I hadn’t, but I understood how easy it could be to reach that stage.
We talked about anything and everything, and we laughed, a lot. I was becoming attached to her, and she knew it. She asked if I wanted a different officer; I declined. Half way through my probation period I was told by a senior officer that I would now only need to see my officer every two weeks. I had been doing well and the concerns of supervising me, exhibited at the beginning, seemed to have lessened. This should have been good news. It wasn’t; I was devastated. I started to think of the time when I wouldn’t be able to see her, and I couldn’t bear it. I thought of the railway track and how much I wanted to end my life. I don’t know how I managed the drive home. I felt numb, yet desperate.
Once home, I couldn’t settle. I sent an email to the probation officer, complaining about never getting any help from CMHT. She phoned me, but I didn’t answer. I knew I wouldn’t be able to talk because I was crying so much. She asked the police to carry out a safe and well check, but they refused. Over the weekend, I sent more emails to my probation officer, threatening anyone she might send to my door. I wasn’t serious but I needed to do or say something extreme so that I could calm down. On the Monday I was arrested and charged with malicious communication. I pleaded guilty. The police said they had a statement from my officer to say she was upset at receiving the emails. The magistrate was sympathetic to my feelings but said he couldn’t allow anyone to send vitriolic comments to probation staff. He sentenced me to 6 weeks in prison.
While in the cell awaiting transport, my probation officer came to see me. She told me that her manager had recalled me to prison to serve the rest of my initial sentence, another 6 months. She also said she had not made a statement and was neither angry or upset at my emails. She thought the whole saga was ‘sad’. Despite the fact that I would have to serve another 6 months in prison, I was happy that she wasn’t angry with me.
After my release, despite the emails, and perhaps proving that she had not been upset the same probation officer continued to supervise me for the seven months extended probation I had been given. I was still attached to her and grateful that I would be seeing her every week. Our relationship went back to the way it was before my arrest and one day, she became emotional and apologised for what had happened. Looking back, I don’t know if she had genuinely wanted to help me or had encouraged my attachment. She game me a lot of information about herself but when I then tried to probe further, she said it was inappropriate. Either way, the thought of not seeing her was more than I could bear. I said it was OK, I didn’t blame her, and it was true. How could I blame her for being kind?
I do question however, why probation officers (and possibly police and prison officers) do not have the kind of awareness training that warns them about attachments so that they can set boundaries. Individuals with BPD can be extremely vulnerable and prone to overplay the smallest act of kindness shown to them. I was told that a forensic psychologist was available to give advice to officers at my probation office. Clearly the advice did not cover those with severe attachment issues.
Since leaving prison, I have been working to raise awareness of BPD and associated attachment issues. One in ten people with BPD end their own lives; I was very nearly part of that statistic.
In 2022, the article was also published by The View magazine:
2. When Therapy Goes Bad: a client’s account of a five-year therapeutic relationship with alisoncalladinetherapy.co.uk Enniskillen & Omagh
I met Alison Calladine, private therapist, through the online Counselling Directory. My mental health had been deteriorating over the previous two years and, as was the norm at the time, there was no help whatsoever for people with BPD. In desperation, my wife and I re-mortgaged our house to pay for the weekly therapy sessions.
When I first met Alison and knew we would be entering a therapeutic relationship, I asked her to never tell me anything personal about her or her family. I promised never to ask. That way, I said, I would not become attached to her. We stuck to that rule, and for the first few years it wasn’t a problem, but then things began to change.
I became oversensitive about some of her statements, taking them personally, ruminating over what she probably saw as innocuous remarks. I felt myself becoming needy and it was making me unhappy. On one occasion I upset her with my ‘hurtful’ (I will come back to this later) comment. She was offended, and I suddenly realised how easy it would be to lose her. I was careful not to upset her again. The relationship was too valuable to me, and I could not take the risk of it ending.
Weekly therapy sessions for five years may seem excessive to some, but it’s not actually that unusual. Whilst it is true that many with BPD dread endings and do not react well when a relationship comes to an end, it is not in itself a good reason for carrying on the somewhat expensive sessions with a private therapist. Most would eventually overcome the initial distress and move on. However, for those of us who have a severe attachment problem, it is not so clear cut.
My attachment to Alison developed after around three years. I tried to hide it from her, partly because I was embarrassed, but also because I didn’t feel comfortable enough to bring it up. Although we had discussed my issues with attachment in detail over the years, we never addressed my feelings towards her. There were clues as to how I felt, and I assumed she knew. One day, I told her that I dreaded the day she would say the therapy had to end. She said it could be open-ended and that, barring a disaster, she would always be there. I wasn’t naïve enough (or was perhaps too cynical) to believe that, but it did make me feel better. I assumed that the issue of my attachment to her was a no-go area, and that was fine with me.
My therapeutic relationship with Alison began to break down the day I discovered (I was told by a third party) that she had moved from Chesterfield to Belfast, without telling me. I checked Alison’s website and the counselling directory and found that she had, indeed, opened up another practice and had already started working from there. I had seen her, online from her practice in Chesterfield, the previous week and had no idea what she was about to do.
Things started to make sense. Until lockdown I saw her face to face at her practice, but then like many others, she changed to online until it was safer, and then operated a hybrid system with both face-to-face and online. I carried on seeing her online. However, after a few months she stopped seeing people face to face altogether. Again, I found out from someone else. I asked her if she was giving up her practice and she replied that she hadn’t thought that far ahead yet. I didn’t know what she meant but tried not to think about it. A couple of weeks later she told me that she had been busy doing other things and that her practice was only a small part of what she did. I asked if she was giving up therapy and she assured me she wasn’t. My reaction at that time, I thought, could leave her in no doubt as to how I felt about her, but we didn’t talk about it.
The feelings of hurt and abandonment, when realising that Alison had moved away from the area, were overwhelming, and my immediate thought was suicide. I can appreciate that this reaction must be difficult to understand by those who do not suffer from this horrible condition. After all, I could still see her online, so what’s the problem? I will try to explain, briefly, how it made me feel (as with everything, no two people’s feelings and experiences are the same). To me, it’s simple; knowing where she was when at work in Chesterfield made me feel secure. Although I would come to know where she worked in Ireland, it wasn’t the same, she might as well have been on Mars. Attachment issues are developed primarily through childhood experiences of abandonment. For me, it’s vital that I know that the subject of my attachment is not too far away. Naturally, I didn’t know where she was outside working hours, and I neither wanted nor needed to.
After finding out about Alison’s move to Ireland I made a 20-minute video explaining how I felt. I talked about my attachment to her and about my thoughts of suicide. Most of the video was taken up by me trying to talk without crying. In all the time I had been seeing her, I had never cried in front of her. I suggested that she spend the first 20 minutes of our next session watching the video and I would join in afterwards. That way, I wasn’t expecting her to do anything in her personal time.
The final session
As arranged, I joined Alison after 20 minutes. I immediately asked her why she hadn’t told me of the move, and that’s when I began to see a side of Alison that I had never seen before. She was defensive and angry. She told me that it was her practice, she could do what she wanted, and it was absolutely nothing to do with me. I said that I wasn’t trying to tell her how to run her practice but that she had misjudged how I would react, given my attachment to her.
Her reaction to this was pure, genuine, shock. She had no idea, saying ‘you said you wouldn’t get attached to me’. I thought this was a rather naïve comment but didn’t say so because I was getting the feeling that she might end the session. It suddenly dawned on me that she hadn’t watched the video, that’s why it was news to her. She said she had experienced technology problems and couldn’t watch it. I didn’t believe her but again, didn’t say so.
I can only describe Alison’s behaviour from then on as nasty and unprofessional. She lost her temper completely and showed a complete lack of empathy or compassion. I realised that this was going to be the final session and, for the first time in five years, I started to cry in front of her. I was distraught; she said ‘look at you, you’re a mess’. I started to get flashbacks to the times I spoke to mental health services, and I felt like I was going backwards. I was torn between trying to hang on to the relationship and maintaining some semblance of self-respect. I ended the session abruptly when she looked at the clock and said nastily, ‘come on, you have 2 minutes left’.
Almost every waking minute for the next week or so was spent thinking about Alison. We still had sessions booked in, so I re-sent the video and paid her another £20. Even though I had already paid her to watch it she still hadn’t seen it and I knew she had no intention of doing so unless I paid her again. I was hoping we could discuss it at the next session.
Although I was hurting, I was becoming angry and started to think of the things she had said and done over the years. Going back to paragraph five of this article, the reason I had offended Alison was because I said I didn’t like it when she yawned when listening to me. We were having a review of how therapy was going. She said she was offended by my comment. I tried to lighten it by asking if I was boring, but she twisted it so that it looked like I thought I was boring. Another time, when there had been a substantial period of silence between us (as happens in therapy) she said, ‘this is your time, you fill it’. I should have realised with these comments that she was getting fed up, but I was attached so I would never have ended it.
After a few days she sent me a message. I assumed she had seen the video because all it said was, ‘I understand’. I wrote back to say that I wanted to cancel all future sessions. At first, I was proud of myself; I had never broken off an attachment before and I knew it was the right thing to do. However, she replied immediately, acknowledging that she had cancelled, and I suddenly realised that I would never speak to her again. I panicked, she was my safety net and I couldn’t face the future without having her there. I emailed her, apologising and asking her if we could resume the sessions. She didn’t reply and I sent several of what I can only call begging emails.
Dear Alison, could we give it one more go please? I am really struggling. Could start a new contract with new boundaries? A fresh start? Please? Best wishes, Sue
She still wouldn’t reply and so I sent a message begging her to reply. I apologised for everything, even though I didn’t know what I had done wrong. It was one of the lowest points in my life. I was embarrassing and humiliating myself. Eventually, she sent a short message saying that she was standing by her decision.
Update
Alison has left her practice in Lisburn and opened up another one in Omagh.
Update
It is now two years since my therapeutic relationship with Alison came to an end. Within a month I had made two important decisions. The first was to find another therapist. Despite how I had been treated by Alison, I came to realise that she was a bad apple and that, with the right person, therapy could work. The second decision was to make a complaint to the BACP about Alison. This was supported by my new therapist, who assured me that it was not usual to stop working with a client just because they had become attached.
My complaint went a long way and then was dismissed. They said that Alison’s comment, look at you, you’re a mess, ‘could have been made in an empathetic and supportive way, or dismissively’. Trust me when I say that it was NOT said in any way except nastily. My complaint about having to pay Alison twice before she would watch the video, knowing how distressed I was, went further. The BACP initially dismissed it, saying there was no contract between us. I pointed out that by accepting payment, Alison was entering into a contract. This was upheld by an external reviewer, but the BACP went against them, dismissing it on the grounds that, although she had accepted payment, she hadn’t actually asked for it. The BACP are known to look after their own. You can see reviews of the organisation at https://uk.trustpilot.com/review/www.bacp.co.uk).
Much of the conversation during the first few months with my new therapist (I shall call her X) was focused on Alison. The loss I felt was incredible, but even worse, her nastiness towards me at the end showed me that she had no respect for me as a client or as a human being. If my self-esteem was low when I met her, it was even lower when it ended. She knew I was having suicidal thoughts. Yes, she informed my GP, but then she dumped me without anywhere else to go. What she did was dangerous. This was Alison’s final comment to me, knowing I was feeling suicidal:
‘I will leave you to assess your own situation, and make the decisions that are absolutely right for you moving forwards.’
In our first session I told X that if I thought I was becoming attached to her, I would end the therapy. I couldn’t go through that again. X was very understanding and assured me that it would be better to have the issue of attachment in the open. Any therapist worth their salt, she said, would not end the client relationship because of their attachment. Yet, this is what Alison told the BACP:
How might this insight (of the disclosure of attachment to me) impact upon our therapeutic relationship? Would I be able to work openly and honestly, knowing Susan was attached to me? Particularly with my knowledge and understanding of how difficult ‘attachments’ are for Susan? Decision. My primary concern was Susan, and it became apparent to me to continue with our therapeutic relationship may cause further distress and suffering to her.’
Clearly, Alison’s primary concern was Alison. She doesn’t know how to deal with someone who becomes attached to her, so she runs away. She has a lot of work to do on herself before treating people successfully with complex emotional needs. Many people are unaware of their attachment issues before accessing therapy and the therapist must be prepared. Otherwise, like Alison, they will cause more damage.
‘Without breaking confidence, I can say that I am not the only person to have fell foul of Alison Calladine. I know of at least two others. The sheer cruelty she has shown by ignoring people’s pleas for help is shameful. I am leaving this blog here as a warning to others.‘
The difference in me since meeting X is enormous. Feeling safe enough to bring everything to the sessions, including my attachment to her (which really didn’t take long) has turned my anxious attachment, almost, into a secure attachment. There is nothing I can’t talk about and between us, we have concluded that I may be on the Autistic spectrum; it makes sense. I won’t be pursuing a diagnosis; I am happy to know why I do what I do and think the way I do. I have a lot to thank X for already.
**If you do decide to be Alison Calladine’s client, PLEASE be careful.**
Remember…
Therapists have the power to create a sense of warmth and safety, but also to hurt, shame and re-traumatise. It’s important you find the right one.
Update
On 1 October 2025, Alison will reach retirement age and start to receive her state pension. Alison also works as a trainer and supervisor, two equally valuable areas of psychotherapy. However, it is in her role as a private counsellor that she has caused most damage and it is my hope that she will take the opportunity to cease working on a one-to-one basis with clients.
It has been said that self-isolation due to the threat of Coronavirus is ‘just like being in prison’. As someone who has experienced both, I feel well-placed to say that, although there are certain similarities, it is not the same!
Let’s ignore the fact that prisoners are currently experiencing their own lockdown, being confined to their cell 23 hours per day, with only one hour to shower and exercise. When people say it’s like being in prison, they most likely mean prison on a ‘normal’ day, i.e., before the advent of the Coronavirus.
One of the main issues of isolation, whether in prison or in one’s own home, is boredom. Those in prison who still have their privileges (any ‘bad’ behaviour can lead to a loss of these) will have a TV in their cell, and books from the library or sent in by friends/family. Many prison wings have a snooker table. Most prisoners have a job or education classes to keep themselves busy four and a half days a week, and there is a gym. Largely due to bad press, prisons are seen as easy, but think about the monotony of having this small set of activities, every week, month or perhaps even years, broken up only by medical appointments and the occasional visit. Then add to this the fact that staff shortages often lead to more in-cell time than is recommended or even humane!
Those on lockdown in the community may also become bored, depending on their particular circumstances. For example, most will be with their own family; those who can afford it are able to order in items to keep themselves busy; they will have no restrictions on online activities, and the hour of exercise can take place in a different area (close to home) each day – as opposed to the same prison exercise yard.
Another problem of isolation is loneliness, although this is not so straight forward. People in prison can be lonely because they have very little contact with their friends and loved ones. Those who do not make friends easily will feel this loneliness even more. For others, prison offers a community spirit that many prisoners crave. They may become institutionalised and, if they do not have a healthy support system in the community, they expect to, and do, return to prison soon after release.
Loneliness in the community, again, tends to depend largely on the individuals’ situation before the lockdown. Those who lived with others continue to do so. Although they may miss certain people, they are not totally alone (although it is possible to be lonely in a crowd if there is no personal connection). However, for those who lived alone and continue to do so, the loneliness may have worsened, especially if they previously had the occasional visit from friends, family members, support workers etc.
The issue that is most common to both people in prison and under community lockdown, is fear and anxiety. In prison, people can live in fear of other prisoners, prison officers, their potential sentence (if on remand) and their physical and mental health. For these people, the sense of being alone, without easy access to information and support, will make that fear/anxiety more extreme.
Those self-isolating in the community due to the Coronavirus will, naturally, be in fear for their own health and that of others. They may even be in fear of loss of life. However, although this fear might be stronger than that felt by prisoners (in a non-Coronavirus environment), there is more access to information and support in the community. In addition, contact with loved ones outside the home, whether by phone or social media, may act as a source of comfort.
All these issues: boredom, loneliness, fear and anxiety, are detrimental to an individual’s mental health. The vast majority of people in prison have some kind of mental health problem which is, more often than not, exacerbated by the stresses of living in prison. Although not as prevalent in the community, most individuals with mental illness whether in prison or community, have suffered from the lack of services caused by under-funding and, to some extent, by a certain amount of apathy and/or stigma among commissioners and the general public.
Regardless of whether self-isolation due to the coronavirus is ‘the same as being in prison’, if the general public think it is, then it may have a positive effect on prison welfare. To some extent, public opinion dictates government policy and it is thought by many that prisoners have a ‘cushy’ life, rather than suffering for their crimes. In law, punishment should be the separation from the rest of society, and not the conditions under which they are made to live. With this in mind, members of the public might realise just how ‘punishing’ it is to be kept away from loved ones; knowing that you cannot be there for them if they need you; the distressing effect of no physical contact with, say, children and/or grandchildren; fear of what could happen next; and the uncertainty of whether life will ever be ‘normal’ again.
The circumstances in which we find ourselves at the moment are unprecedented but appear to have brought out the best in people. Life has slowed down considerably, giving them time to re-evaluate what is important. Perhaps this can be capitalised upon when reviewing prison reform.
Sue Wheatcroft is Expert by Experience at Revolving Doors Agency in England (LINK http://www.revolving-doors.org.uk/). She is also a Research Assistant in the national Cancer Care in Prison Study (How is cancer care best provided to patients in English prisons? Assessing the disease burden in the prison population, experiences of diagnosis, treatment and support, and of receiving and providing cancer care LINK: https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/165253/#/)
Book: Worth Saving: disabled children during the second world war
Book chapter: Holiday camps, castles, and stately homes: the residential option for the evacuation of disabled children during World War II, Sue Wheatcroft
Book chapter: Cured by Kindness? Child Guidance Services during the Second World War, Sue Wheatcroft
Journal article: Children’s Experiences of War: Handicapped Children in England During The Second World War
1. Book: Worth Saving: disabled children during the second world war (2015)
This book contains the first detailed study on the experiences of disabled children in England during the Second World War. It examines the lives of those who were evacuated into residential special schools within the reception areas and compares their experiences with others who, for various reasons, were not evacuated, who returned home early, or who spent time in hospital. Through the use of official documents, newspapers and personal testimony the book shows that for many disabled children the evacuation was a positive experience but one which depended largely on the attitudes of the authorities and of the general public, and perhaps more importantly, the attitudes and quality of the teaching and nursing staff, who were responsible for the children on a daily basis. The book reveals how the government evacuation scheme worked for certain groups of disabled children and how it failed those most vulnerable. Worth saving serves as a social commentary of a time when attitudes towards disabled people in general were changing, and demonstrates the impact that wartime conditions had on special education both during and after the war. It introduces a new area of research to a range of disciplines including Disability History, Childhood, Social Policy, Special Education, the Voluntary Sector, and the Second World War/Evacuation and is written in a style that is accessible both to academics and to the general reader.
2. Book Chapter: in ‘The Blitz and its Legacy: wartime destruction to post-war reconstruction’ (2013)
Introduction: Disabled Children – Contested Caring, Anne Borsay, Pamela Dale;
Chapter 1: Club Feet and Charity: Children at the House of Charity, Soho, 1848–1914, Pat Starkey
Chapter 2: Insanity, Family and Community in Late-Victorian Britain, Amy Rebok Rosenthal
Chapter 3: The Mixed Economy of Welfare and the Care of Sick and Disabled Children in the South Wales Coalfield, c. 1850–1950, Steven Thompson
Chapter 4: The Question of Oralism and the Experiences of Deaf Children, 1880–1914, Mike Mantin
Chapter 5: Exploring Patient Experience In An Australian Institution For Children With Learning Disabilities, 1887–1933, Lee-Ann Monk, Corinne Manning
Chapter 6: From Representation to Experience: Disability in the British Advice Literature for Parents, 1890–1980, Anne Borsay
Chapter 7: Treating Children with Nonpulmonary Tuberculosis in Sweden: Apelviken, c. 1900–30, Staffan Förhammar, Marie C. Nelson
Chapter 8: Health Visiting and Disability Issues in England Before 1948, Pamela Dale
Chapter 9: Spanish Health Services and Polio Epidemics in the Twentieth Century: the ‘Discovery’ of a New Group of Disabled People, 1920–70, José Martínez-Pérez, María Isabel Porras, María José Báguena, Rosa Ballester
Chapter 10: Cured by Kindness? Child Guidance Services during the Second World War, Sue Wheatcroft
Chapter 11: Education, Training and Social Competence: Special Education in Glasgow Since 1945, Angela Turner
Chapter 12: Hyperactivity and American History, 1957–Present: Challenges to and Opportunities for Understanding, Matthew Smith
4. Journal Article: in Twentieth Century British History, Volume 19, Issue 4, 2008, Pages 480–501, (now Journal of Modern British History)
Children’s Experiences of War: Handicapped Children in England During The Second World War
Abstract
The experiences of children during the Second World War have attracted considerable attention, both scholarly and popular. Not all children however, have received equal attention. Handicapped children are conspicuous by their absence from all types of literature, both on evacuation and on children’s experiences of the Second World War. This article restores these children to the story of wartime England and assesses their experiences. It examines the plans that were made for their evacuation and how they were carried out, and compares their lives, both individually and institutionally (i.e. in the various types of ‘special’ school) with those who, for various reasons, were not evacuated. It also compares their experiences, to a lesser degree, with those of their non-handicapped counterparts. The article argues that for many handicapped children it was a positive experience but one which depended on specific aspects, such as the attitudes of the authorities and of the general public, and perhaps more importantly, the attitudes and quality of the teaching and nursing staff, who were responsible for the children on a daily basis.
2. Speech: Rethink 50th anniversary event (House of Parliament, 2022)
3. Keynote Speech: Derbyshire County Council Consultation (Chesterfield, 2024)
4. Keynote Speech at Comensus Conference (UCLan, 2024)
5. Speech: Service User Voice at HIEM/Mental Health Alliance Learning Event, (March 2024)
6. Joint Keynote Speech at HIEM/Mental Health Alliance Learning Event, Nottingham (March 2025)
7. Speech at the Mental Health & Wellbeing Faculty research theme Showcase, Stafford (24 September 2025)
1. Speech: Supreme Court (2019)
Delivered at the Empowering Women, Transforming Lives conference at the Supreme Court, on 4 September 2019:
I was in segregation and had nothing. No clothes, no radio, no writing materials and nothing to read. What I did have was a razor blade. I wasn’t often strip-searched because I didn’t have a substance abuse problem, so I was able to smuggle it in. I didn’t intend using it; I had it ‘just in case’. But after several hours of staring at the wall and listening to the shouting and screaming coming from the other cells, I suddenly felt desperate. I cut my wrist. It wasn’t a suicide attempt. I didn’t want to die but doing something extreme made me feel better. I didn’t understand it but couldn’t seem to control it. The cuts were deep and there was a lot of blood. I let the blood drip onto the table and then used it to write on the walls.
Deputy manager Paul (not his real name), came in and told me to wash it off. I refused. He took hold of my head and pushed it onto the bloody table. ‘Now are you going to take it off?’ he said, nastily. ‘No!’ I replied. He pushed my head into the corner of the table until it was against the wall. There was blood in my hair and on my shirt. I wanted to stop him and get him off me. I picked up some congealed blood from the table and wiped it on the side of his shirt. He got hold of my arm and put it up my back. ‘One move and I will show you a whole new world of pain’, he said. I didn’t move. He told the officers to leave the cell and said he would be the last to leave. ‘I bet you would love to go for me now, wouldn’t you?’ he whispered, but that was the last thing on my mind. I didn’t say anything. He said, ‘thanks for the assault’, and left.
A nurse came to see me. The wound was quite deep, so she put a couple of steri-strips on, and then dressed it. The next morning, I was given my belongings. I had a shower and was grateful for the clean clothes.
Paul had put me on report for throwing congealed blood at him and so endangering his health or personal safety. My blood could have been contaminated, the adjudicator told me, and it had caused Paul considerable distress. I looked at Paul; he certainly didn’t look distressed. In fact, he seemed to be grinning at me. I pleaded not guilty because I had not thrown it at him; I had merely wiped it on his shirt in order to stop him hurting me. There was no malice intended and I didn’t feel I was being reckless with his health. I was found guilty, of course, and received more time in Segregation.
You may be thinking ‘why didn’t she just try and wash the word off and all that could have been avoided’. That’s what the officers said afterwards. I had caused myself all that grief because of my bad behaviour. I have Borderline Personality Disorder. Therefore, I am an attention-seeker. The only person who tried to understand was the prison psychologist, but she didn’t have time to treat me. Her job, she said, was to keep me out of segregation.
By the time of the incident with Paul, I had already been in segregation a number of times. Out of the 12 months I spent in this particular prison, a total of 3 months was in healthcare and 5 months in segregation. My way of coping in prison was to draw pictures and write stories on the walls of my cell. Some of them were funny, some were dark, and some were extreme. Everything I was feeling at the time was displayed on those walls. I understand now how ill I was, but at no time did anyone want to know what they meant or why I needed to do it. It invariably led me to segregation, but I never thought of the consequences. It was a compulsion, and the only way I could find to calm myself down.
In segregation, my behaviour became more extreme. As a punishment for the graffiti, I had all writing materials confiscated. Instead, I used coffee to write on the walls. The way the coffee made the letters drip down the wall made the cell look almost gothic. I felt safe, cocooned, there was hardly a space left on the walls. Eventually, I was taken to another cell and left there while my old cell was cleaned. I had no belongings at all, and the water was turned off in case I tried to flood the cell. All I had was the water in the toilet and a toilet roll. I wet the wall, made a word out of the toilet paper, and stuck it to the damp wall. I won’t tell you what the word was, I think you can guess.
Prison is an extreme environment and it brings out extreme behaviour in people. Ironically, two of the most compassionate officers I met were the two female officers in the cell at the same time as me and Paul. But they were afraid of him when he was in that mood. He could be very jolly when things were going well, but he had a dark side. His officers loved him, though, he always backed them, whatever they did.
I will never forget my time in segregation. Not because of my experience. I feel I gave as good as I got. But some of the women seemed to have given up. And this is why, when I came out, I started my volunteer work. I have set up my own support groups in Derbyshire for people with Borderline Personality Disorder. And I have done a considerable amount of work for the Revolving Doors Agency, including contributing to the Bradley Report review, 10 years on. One thing that that many ex-offenders have in common is the desire to help those still inside and through the gate. As part of the Health and Justice Lived Experience Panel, I have been back into the women’s estate to speak to the women about not giving up. I want them to know that their life means something and that they can still achieve their ambitions, because they are worth something. This was part of the pre-release skills project that we devised and piloted, and that is now embedded at the prison.
I would like to finish with one memory I have of my time in segregation that I am sure will stay with me forever. A woman a couple of cells away from me was due to go to court for sentencing and had been fretting about it for days. Not because of her case but because of her elderly grandmother, who was making the long trip to see her in court. But on the day, the officers never came to fetch the woman. She asked the senior officer, time and time again, what was happening, but he told her to shut up. I heard him laughing about it to his colleagues who, I think, he was trying to impress. I remember the woman sobbing, saying over and over, why are you doing this to me?’ It was heart-breaking. I never knew her name and I never saw her but she, and others like her, is the reason why I will never give up trying to bring change to the criminal justice system.
Thank you
2. Speech: Rethink 50th anniversary event (House of Parliament, 2022)
My speech
Thank you Mark and thank you for inviting me here today.
In 2015 I suffered a mental health crisis that led to a diagnosis of borderline personality disorder, or BPD. In the UK this is also known as emotionally unstable personality disorder, or EUPD. As the name suggests, it is a disorder of the emotions. When in crisis, we struggle to manage our thoughts and feelings and find it difficult to self-soothe or calm down. We need to do something extreme so that we can re-set our emotions and behavioural patterns. Some people self-harm, others commit an offence and some end their own life. 7 in 10 people with BPD self-harm and 1 in 10 end their own lives. 1 in 10! BPD is a severe mental illness.
In 2017 I was in recovery. It had been a rough couple of years during which time I had received no help at all for my mental health problems from statutory services. In fact, by trying, or should I say, begging for help and being refused, my mental health deteriorated, with disastrous consequences. I went to prison and my disabled partner was placed in a care home. On leaving prison, I found a private therapist, and my recovery began. I started thinking of others with BPD. Not everyone can afford to go private, and I couldn’t bear the thought of them going through what I had, so I decided to start a support group, and that’s when I first came into contact with RETHINK Mental Illness. Through their Derbyshire Peer and Recovery Support Service, I managed to set up the group and keep it going. We will celebrate our 5th anniversary in October. Over 250 people have passed through our service, from all over the UK and several from overseas. RETHINK Mental Illness have supported us since the beginning, and I can’t thank them enough.
I have also worked with RETHINK Mental Illness on their national lived experience advisory board and community’s advisory panel. Having such faith placed in me has spurred me on to do more and I am now a member of the East Midland Academic Health Science Network PPI Senate and the Revolving Doors Agency. I am also a fellow of the Fair Access to Justice Institute and am on the research team for the University of Central Lancashire’s Offender Personality Disorder Pathway Higher Education Programme. And this brings me to what I believe is imperative for the future of all mental health treatment: adequate education and training. People talk about trauma-informed care and of course, this is essential, but sometimes even that’s not enough. A real understanding of the condition you’re treating is vital.
The vast majority of people with BPD have suffered some kind of childhood trauma. This could be mental, emotional, physical or sexual abuse. Sometimes, it is all of these. When these children grow up, they often face stigma from statutory services, who see them as mere attention-seekers. But that’s because they don’t understand. The number of professionals, whether it be in health or criminal justice, who are openly hostile to those with BPD is incredible, and wrong.
Before my mental health crisis, I was an academic in history, and a published author. Now, I am a campaigner for mental health and women in prison. I want people at all levels, whether strategic or front line, to look beyond what they are seeing and to understand why people behave the way they do. What has happened to them?
I was 55 years of age when I was diagnosed. Before that, I hid how I felt because I didn’t know anyone else felt the same way. I thought I was weird, a freak. I had severe abandonment and attachment issues and I was ashamed and embarrassed. But I would have given anything to have someone to talk to about how I was feeling. Someone who understood. When I told my support groups members, I was coming here today they asked me to pass on a message to RETHINK Mental Illness. Thank you so much for enabling our support group to exist; for helping to provide a space where they can meet each other without feeling judged. But our group is not a substitute for professional help.
Despite all I have said, I have hope for the future. We have an excellent voluntary sector in this country. We have an army of volunteers willing to help. Peer support is increasing and becoming more valued. And then there’s the next generation; students of health and criminal justice. I have carried out training sessions for some of these groups and they are so willing to learn and to understand. I encourage them to become the kind of professional they want to be, rather than following those who, probably through no fault of their own, have become cynical and jaded.
People with BPD don’t want better care than anyone else. They want parity, and they want to be treated right. No condition should be stigmatised, and no individual should be discriminated against, for any reason. I hope we can all work together to bring about change.
Thank you
Note
Sajid Javid resigned shortly before the event and was replaced by Secretary of State for Care and Mental Health, Gillian Keegan MP.
Unfortunately, the Shadow Minister for Mental Health, Dr Rosena Allin-Khan MP was taken to hospital shortly before the event and was unable to attend.
Speaker of the House of Commons, Sir Lindsay Hoyle, attended the event along with several other MPs.
Mark WinstanleyGiving my speechWith Gillian Keegan
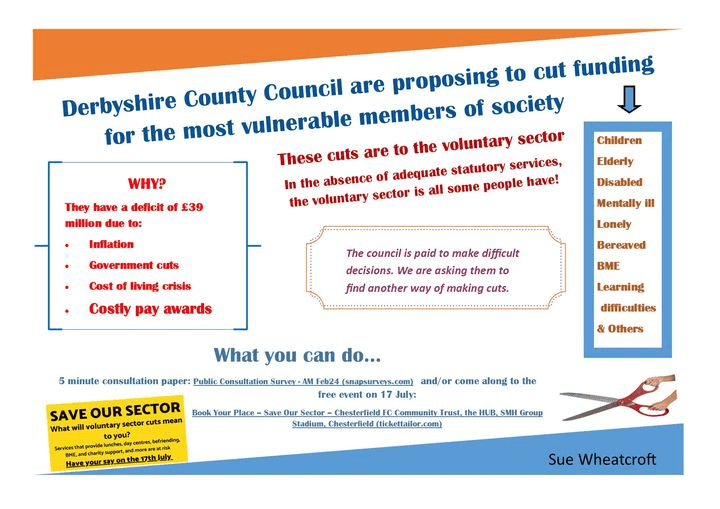
3. Keynote Speech: Derbyshire County Council Consultation
A DVA event,SMH Group Stadium Chesterfield, 17 July 2024
I’ve known about the proposed cuts to the voluntary sector for a while, but when I was asked to speak here today, I thought I’d best delve deeper and get my facts straight. It seems that adult day care centres, lunch clubs, and many of the other vital assets, that people have worked hard to establish and maintain, are in danger of closing. If the proposals go ahead, it will inevitably result in even more suffering for those most in need.
Cuts do have to be made and I don’t envy those whose job it is to make them. But that’s what this consultation is all about, isn’t it? To present to the decision makers at Derbyshire County Council what people think about their proposals, in a respectful way of course.
Like many, I am proud of our voluntary sector and I’m proud to be a part of it. I have several hats, but the most important is the support group I run for those who have borderline personality disorder. There are many groups like mine, who rely on the support and guidance of the larger voluntary sector organisations. Cutting their funding will effectively put an end to many of the smaller groups.
I would like those who are considering these cuts to understand the true value of community and voluntary groups. Not everyone has support in the form of family and friends, and most cannot afford to go private. Until they have adequate services to rely on, these groups can be the only support someone has. But they’re not just social groups that gather for coffee and a chat. For many, it’s the first time they’ve been able to meet others who struggle with the same or similar difficulties.
My support group can’t provide therapy, and our members still need to access services where they can, but I must say, the kind of support they give each other is amazing. They’ve found a sense of belonging, where they’re not judged or ignored. This might not mean a lot to people who are not over-sensitive and paranoid, or don’t often feel the need to self-harm, or don’t act like a child but can’t seem to control it, but our members recognise how difficult it is to manage these emotions and they praise each other for not doing those things. They encourage each other to find distraction techniques and to keep themselves safe.
We provide a website, newsletters, zoom calls and Whatsapp groups, but we also encourage them to develop their own networks between themselves, and many have. They go bowling and meet for picnics or for walks. They want to help themselves and each other; they just need that extra help that a community group like ours can provide.
There are many community groups around Derbyshire doing amazing work. If their funding is taken away, what’s left? My guess is that the long-term consequences on people’s health, and therefore the financial cost on the taxpayer, will far outweigh any money that will be saved by devastating the voluntary sector. Please remember that we who run these community groups don’t get paid for what we do. We’re volunteers, who do it because we’re passionate about helping people. But we can’t do it alone.
Without over-simplifying the issue, isn’t it a matter of priorities? Shouldn’t high salaries come second to ensuring that people have their basic needs met? And by this I am including befriending to prevent loneliness, counselling for the bereaved, day care centres for disabled children and adults, and for older adults. And the many other networks and services that we ourselves may not need right now. But who knows what help we might need in the future!
I don’t usually use the quotes of American politicians, and don’t worry, it’s not Donald Trump, but I think this one is relevant here. You’ve probably heard it before:
“It was once said that the moral test of government is how that government treats those who are in the dawn of life, the children; those who are in the twilight of life, the elderly; and those who are in the shadows of life, the sick, the needy and the handicapped.”[1](disabled)
What I would like to say to the decision makers at Derbyshire County Council is, please take a step back and think of the consequences of what you’re doing to the people of Derbyshire. By cutting discretionary grant funding to voluntary and community organisations you will, in effect, be reducing the most vulnerable in society to collateral damage. The money you save would be short-term but the problems it could present are long-term and far reaching. Please take note of the views gathered in this consultation. Search your conscience and work together to find a way that does not target those most in need.
Thank You!
[1]At the Hubert Humphrey Building dedication, Nov. 1, 1977, in Washington, D.C., former vice president Humphrey
DVA event, SMH Stadium, Chesterfield, 17 July 2024
4. Keynote speech at Comensus Conference (UCLan, 2024)
Speech
Thank you, Mick, and thank you to Comensus, for inviting me here today.
Explain outline of speech (on slide)
Seven years ago, I was sitting in a prison cell, dreaming about what I would do when released. I had a relatively recent diagnosis of borderline personality disorder (BPD) and had quickly learned just how much stigma and misunderstanding surrounds the diagnosis. The judge in my case knew nothing about it and was persuaded by my local community mental health team that it was untreatable and that neither they, nor the probation service, were willing to supervise me. This resulted in me being given a custodial sentence rather than a community or suspended sentence.
I learnt a lot about injustice in prison and how both the mental health and criminal justice systems were failing people, and I wanted to do something about it. I wanted to help people. The thing was, I had no idea how to go about it. Like most people in prison, I knew nothing about experts by experience and how they were working to bring change. As far as we were concerned, no-one cared about us other than our own families and friends.
I have decided to include my prison experience in my speech because health and social care is a vital part of it. Women especially, experience poor physical and mental health and many are living with trauma. I look on this part of my life, and the events leading up to it, as my crisis period. The time since my release I see as my recovery period.
I know there are a lot of people here that are heavily involved in patient and public involvement, and I wouldn’t presume to know more about it than any of you. I want to share my story with you to highlight some of the different opportunities that I found, and also, some of the pitfalls.
So, back to my prison cell . I would start a support group, I thought. Having never attended one myself, I thought they were all run the same, like AA . Hello, my name is Sue and I have borderline personality disorder . Of course, it didn’t turn out like that.
After my release, I was put in contact with someone at Rethink Mental Illness, who helped me to set up the Derbyshire borderline personality disorder support group. It’s now in its seventh year and has helped over 400 people, including several from overseas.
I have always been proud of the group, of course. It provides a space where like-minded people can come together and support each other. But I wanted to do more. I wanted to get involved in bringing change, so that our group will be supplementary to, rather than in place of, adequate treatment.
Through Rethink, I was introduced to Healthwatch, and joined their advisory panel, which was made up of experts by experience. Through my work there, I was put in touch with an agency in London, who were working for prison reform. And through them, I became part of the East Midlands Health & Justice team.
All this happened relatively quickly, but I was enjoying it. I was convinced that I was making a difference, and in some ways, I was. I went into prisons to interview people with cancer on their experiences of treatment. I co-produced and co-delivered a pre-release skills course in a women’s prison and then developed a best practice guide.
I even went back to the prison I was in. I hoped I would see the officers who had, so often, accused me of being an attention-seeker. I wanted to say ‘see, you were wrong about me!’. Unfortunately, or perhaps fortunately , I didn’t see anyone I knew.
I learnt a lot from going into the various prisons. As a prisoner, I could only see one side, which wasn’t always positive. But going in as a researcher, or to deliver a skills course, gave me a different perspective. I saw how overstretched the officers were, as well as the serious lack of communication between each sector of the prison. My colleague and I sat waiting for over an hour for an escort to take us to the interview room because the reception staff were busy and forgot to ask for them.
I thought back to a time I had asked an officer to take me to the visiting room. He said he would send someone to fetch me, but they never turned up and I missed my visit. I took it personally and thought they had done it on purpose. But sitting there waiting for an escort, I could see how easily it could happen.
My biggest achievement at that time, I felt, was being part of the east midlands prison partnership board. It was a partnership between the NHS and the criminal justice system, two organisations I felt passionate about. As a board member, I was able to bring items to the agenda, see them minuted, and then actioned. This was true co-production.
I told the board of my experience in prison after I had fell and dislocated my shoulder. I was left in pain for 5 days before they allowed me to go to hospital to have it corrected.
This kind of lived experience can be particularly useful for those at the top, who are unaware of what goes on a daily basis.
On the board was a prison director, who said that my case must have been an isolated incident. It would never happen in any of his prisons, he said. I suggested, politely, that someone in his position would not necessarily be told of such rudimentary matters.
I knew this director didn’t like someone like me being on the board. Whenever I spoke, he either sighed loudly or looked pointedly at his watch. Fortunately, the Chair of the meetings was the one who had invited me onto the board and made sure I had my say. It was agreed that I, and the rest of the health and justice panel, should carry out research into the subject, and this led to another best practice guide for prisons; this one on escorting prisoners to and from the local general hospital.
At another board meeting, I brought up the issue of physical abuse by officers on prisoners. I told of my own experience of this and was advised by the director to bring an assault charge against the officer. I was surprised at this and thought that maybe I had got the director all wrong. But then he followed it up with, of course that would mean that you wouldn’t be able to carry on with this board because it would be a conflict of interest. I told him that I could do more good by staying on the board, but thanked him for his ‘concern’.
In time, the work I was doing started to affect my mental health. I couldn’t risk another crisis and so decided to take stock of which jobs I enjoyed and which ones I found too stressful. Also, which organisations truly believed in PPI, and which included people with lived experience merely to tick a box to say they did? Was I valued, or was I being used.
Firstly, Healthwatch. Several times they asked me to represent them at multi agency meetings regarding crisis plans, but each time, the police would veto it, saying it was inappropriate because of my criminal record. After a while Healthwatch, understandably perhaps, stopped asking, and so I left.
The agency in London got me involved in several things, which I enjoyed. For example, the cancer in prison project. This had been run jointly by a major cancer charity and a university in the south of England, and it led to me, and the two other lived experience members involved in the project, contributing to a published academic paper.
But then I discovered that the agency had charged the project funders an enormous amount of money just to provide our names. The three of us were paid just £45 per day by the agency and, although I didn’t start this work to make money, I didn’t like the idea that the agency was using me to make money for themselves. So, I left. Around the same time, I left the prison partnership board. I felt that I had gone as far as I could and there were others on the health and justice lived experience panel that could take over.
When I was first asked to get involved in this kind of work, I felt grateful for being asked and vary rarely turned anything down. But I wasn’t always fully prepared. For example, the males I interviewed about their cancer treatment were all sex offenders and were serving long sentences. I went there with the idea that they were human beings, and I had a job to do. But, in subsequent weeks I felt guilty.
I had joked with some of them, mainly as an icebreaker so they would feel comfortable. My colleague and I got the information we needed, but several times we had to stop them from talking about their offences. I ruminated about this for a long time after, the guilt came from the knowledge that I had joked with someone who, if defined by their crimes, were monsters. In a way, I felt like I had let down their victims.
But I learned a lot from that experience. Self-care and self-compassion are vital in this kind of work, whether we interview someone else or share our own stories. If you’re new to PPI, I would advise being selective in what you take on and beware of tokenism & exploitation. Consultation and Informing can be just as valuable as coproduction, but it’s important to recognise what you are contributing. Organisations should not use you to tick the co-production box if that’s not what’s happening. Honesty, trust and transparency are vital. Equally important – you should be enjoying what you do.
As you will know, much of PPI work is voluntary. Payment can be a contentious subject, but I think it’s a matter of personal choice. I was recently asked by my local police to do a training session on personality disorders for some of their 999 call handlers. I was interested, of course, and would have done it for free. But then I was told that, although it’s usual to provide payment for this kind of work, as they do with the carer’s association, the hearing and sight impaired, and the various other organisations they invite, they could not pay me because there was no budget for personality disorders. I felt insulted on behalf of my community. Why were we being treated differently? So, I regrettably declined, but said that I would make myself available as soon as the budget allowed for it.
After giving up so much of my work, I had more time to concentrate on my writing. I was, and still am, an academic. Before prison, I was a historian and wrote a book about disabled children during the second world war. But after my crisis period, my work became all about prison reform and mental health. I had several articles published, including one in Custodial Review, a magazine for the police and prison services.
I decided to write an article for an online journal meant for probation practitioners and researchers. I wrote about the importance of boundaries in the probation officer and client relationship, and it was published in 2021. As an introduction to the article, the editor wrote,
In this issue, we have a challenging article from a service user, Sue W. It does not make for comfortable reading but Sue’s analysis of what could and should have been done differently in her supervision – not only by probation but also by community mental health services – is eloquent, and she argues that achieving the right balance between empathy and professional distance requires a sophisticated level of skill and awareness.
I was proud of the article and pleased with how it had been received by the editor. But a couple of weeks after its publication, a colleague told me they couldn’t find it. The journal was online but without my article. Fortunately, I had downloaded the issue as soon as it had been published so I compared that with what was online now. They were the same in every way, except that my article had been withdrawn. I phoned the editor but was told she didn’t want to speak to me.
To this day, I don’t know why that happened, but it had an enormous effect on me at the time. Fortunately, since leaving prison I have been seeing a private therapist and so was able to discuss it with her. She helped me to move on from it and advised me to stick to the voluntary sector for a while. I wrote a few blogs and participated in health and justice panels, podcasts and webinars. And I became a reviewer for Research Involvement and Engagement, a coproduced journal, which focuses on patient involvement and engagement in all stages of health and social care research.
Then, in July 2022, I delivered a speech at Rethink’s 50th anniversary event held at the Houses of Parliament. The event was attended by Gillian Keegan, who at the time was the Minister for Mental Health and Social Care. She listened to my speech, was polite and encouraging and said that yes, things had to change. She wanted to get involved, she said, but I was sceptical, and rightly so. Two months later she moved into a new post, and we never heard from her again.
I decided to try a different way of raising awareness. Every single day of my time in prison I had written something about prison life. What I saw and how I felt. I talked about other prisoners, the officers, healthcare (which was run by the NHS rather than by the prison) and the prison system itself. How it worked on a daily basis. I had kept everything and now thought it was time to turn it into a book, which I published on Amazon at the beginning of 2023. After that, I wrote about the health and justice system from my perspective, using my case as an example, and I published that at the end of 2023.
Looking back at the work I have done, a lot of it has been by consultation and sharing information, as well as co-production. Here’s a few more examples…
Slides
Conclusion
For those of you who are here today from organisations that already include people with lived experience, or are thinking of doing so, please value them. Their insight is extremely important in making services successful. And please look after them. This kind of work can be enormously helpful to someone who is trying to make sense of their own experiences, but it can also be stressful and exhausting.
Like most people working in PPI, I am passionate about the work I do. It’s helped enormously with my recovery, and I have learnt a lot. And I think I have managed to find the right balance in order to stay psychologically safe. I’ve learnt what my limitations are, the importance of self-compassion and of showing compassion to others, and to try and see both sides of an issue.
But we’re always learning, aren’t we? And I’m looking forward to learning about other people’s experiences and different methods and experiences of PPI at this conference. There are some great speakers lined up, so I hope you all enjoy it as much as I know I will.
Thank you!
5. Service User Speech: HIEM/Mental Health Alliance learning Event, March 2024
Hello everyone,
When I was on a psychiatric unit, I thought people didn’t care. My work with the Collaborative, and events such as this, shows me that people do care and want to work towards reducing the need for restrictive practices
My first time on a psychiatric unit was in the 1970s. I was14 years old and on an adult ward. Several things stand out from that time but the most horrific was seeing an elderly severely mentally ill man in the breakfast room being physically restrained and forcibly fed. It was done in a brutal way and was extremely distressing for the patient, who was left with a bloody nose and mouth. I remember it as if it was yesterday. What I also remember is the lack of any kind of reaction from the other patients. I was transfixed and distressed by what I saw but everyone else looked away and carried on with their own breakfast. I came to realise that this kind of behaviour was accepted.
My next stay on a psychiatric unit was just over 40 years later, in 2015. I didn’t see anything as horrific as that, but I experienced physical restraint myself after having an argument with another patient, and I saw others being restrained. Thankfully, safer handling techniques were used, and no-one was injured. But again, other patients seemed oblivious to what was going on, even though they could hear the commotion, and it seemed to be accepted.
At no time, during both my stays in hospital did anyone ask for the patients’ opinion on anything. Now, 7 years after my last experience, I can see that things are changing. Patients are getting more involved in their own care and trust is being built.
For me, projects like this are important because they show patients and other service users that their opinions do count and can make a difference.
6. Joint Keynote Speech: HIEM/Mental Health Alliance, Nottingham (March 2025)
Hello everyone,
I’ve been involved with the mental health programme, since 2021 and have taken part in all 4 of these learning events. I’m currently in the Preventing Suicide and Self-harm community of practice and have recently been involved in co-producing a video on compassionate phrases. We all know how stigmatising language can be, but it can also be a force for good. By using clear, positive language we can turn a statement of distress from being viewed negatively to a request for help. For example, from attention-seeking to seeking support.
When I first joined the mental health programme, I was part of the reducing restrictive practice workstream. At the first event I spoke about my experiences on a psychiatric ward, back in the 1970’s, when I was a young teenager. I compared it to my experiences a few years ago. A gap of 50 years, which makes me feel very old!
Obviously, a lot has changed in that time, but for me, one of the changes that stand out most, is that I now have a voice and a place to express how I felt as an in-patient. And it’s not just because I’m older. Despite my age, I was put on an adult ward and saw the brutality of force-feeding and restrictive practices. There was an acceptance by the patients, and their families, because they couldn’t do anything about it. They didn’t have a voice. I remember those patients as if it was yesterday. I’m sure none of them could have imagined a time like this. A co-produced learning event where both former patients and staff get together to discuss their experiences of being on a ward, whether as a patient or staff member, so that we can continue to work together and improve safety.
Being part of something like this, where we discuss and listen to issues that are potentially triggering, means that our own well-being should be protected. I know from experience that not all organisations are aware of this, and the mental health of those with lived experience can suffer as a result. This is not the case with the mental health programme. They recognise their duty of care; it’s one of their principles of involvement. From the beginning, I’ve been aware that there’s someone I can talk to if I have a problem, and after every meeting, we’re given the chance to discuss how it’s gone and how we feel. We don’t always take this up; the point is that the help is there if we need it.
Another stand-out moment for me in my work with the mental health programme, has been the webinar I co-produced with staff members Kay and Deborah.
Involving people with lived experience to transform mental health services.
Representing all of us lived experience members, I discussed what we can offer by doing this work, and what we can gain. We can offer commitment as well as our individual insight and skills, such as facilitating, leadership and public speaking, and we can gain new and improved skills.
But the rewards are much more than that. We can benefit from improved mental health (speaking out and helping others can be massive in this respect). A sense of equality (by working together as equal partners). A sense of making a difference and helping to improve services for us and others. And, of course, increased confidence and self-worth.
In other words, involving people with lived experience, if done correctly, can be a win-win situation.
Thank you for listening.
7. Speech at the Mental Health & Wellbeing Faculty Research Theme Showcase, Stafford, 24 September 2025